For the developed world
Although it is known that the distribution and processing of food can lead to a
significant loss in nutritional quality, there are few instances where present
evidence suggests there is a need to change current practices. There is very little
evidence for nutritional deficiencies. In those cases where public health
authorities have thought there is a potential problem, food supplementation with
nutrients is a commonly adopted policy. The use of nutritional supplements is
widespread. Whilst the focus of current interest is on the need to consider
nutrients and other phytochemicals as protective against the development of
disease in later life, the levels of intake that may be necessary to optimise
protection are far from resolved at the present time.
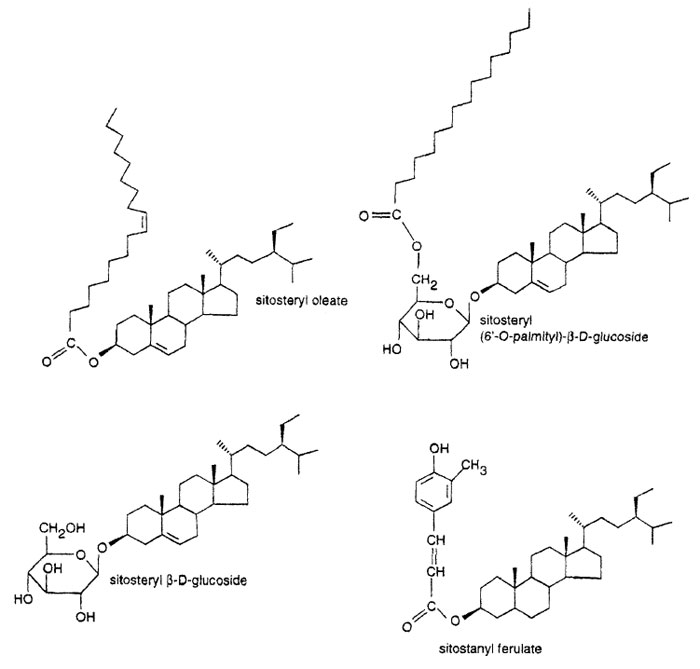
Fig. 7.1 Structure of plant sterol and stanol esters.
The only plant-derived food product on the market where nutritional health
benefits are claimed (as opposed to implied) is the enrichment of margarines with plant sterol and stanol esters for the reduction in plasma cholesterol levels
(Fig. 7.1). These products do not require the development of specifically bred
plants since it is possible to extract stanols and sterols from existing plants
(albeit in the case of the stanols from the bark of a tree) for use in their
manufacture.
Experiments with plant stanolesters were shown to lower serumcholesterol
consistently by about10–15%and LDL-cholesterol by about 20% in patients
with high serum cholesterol levels as well as in normal individuals [16, 17]. Similar
effects have been seen with plant sterolesters but at least 1g/day of plant sterols
need to be consumed [18]. Consequently they require extraction and addition to
foods.
Fig. 7.1 Structure of plant sterol and stanol esters.
Plant sterols can be in the free form or predominantly esterified with long
chain fatty acids or with phenolic acids as in rice-bran oil (ferulate) and shea
butter (cinnamates). Sterol estersare better absorbed than the free sterols and
most sterol esters are hydrolysed to the free sterolsin the intestine.
As campesterol esters are better absorbed than sitosterol esters, serum levels
of campesterol could rise to those levels that are found in the very few people who suffer toxic symptoms from phytosterolemia. Thus there may a benefit in
increasing the sitosterolto campesterol ratio in plants.
The ideal situation would befor sufficient sterols to be present in our diets to
ensure that plasmacholestero levels are kept reasonably low without the need to
buy a specific functional food, and that they would be in a fat soluble form for
effective uptake. The evidence favours in increasing order of preference the use
of:
- plant sterolesters with low campe sterol contents
- sterol esters from tall oil (derived from pine wood) which havea higher
stanol content than edible oils
- plant stanolesters.
A vegetable oil rich in plant stanols, especially in sitostanolesterified with
polyunsaturated fatty acids, would also have the benefit of being less susceptible
to oxidationat frying temperatures than the sterols. The potential health benefits
of this class of bioactive compounds are unlikely to be met by the use of
classical plant breeding methods but genetic engineering could make these
targets feasible.