Gut helminths
Gut helminths
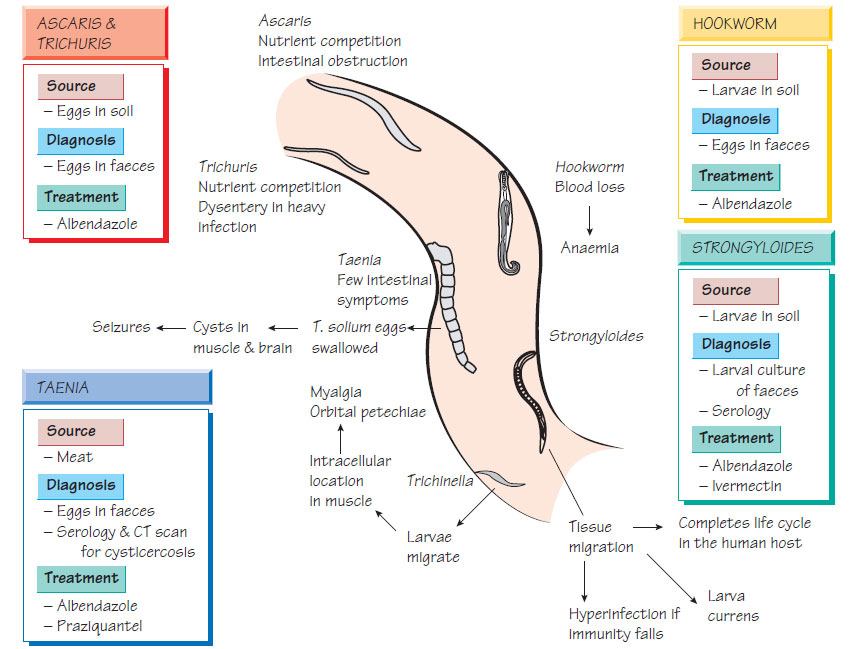
Infection by nematodes (roundworms), Ascaris lumbricoides and Trichuris trichiura, or hookworms, Necator americanus and Ancylostoma duodenale, is prevalent in developing countries.
Epidemiology
Adult Ascaris are found in the intestine; the female worm produces up to 2000 eggs per day. The eggs survive in the soil where they mature into infective forms that can be ingested. After hatching in the small intestine, the organism undergoes a migratory cycle through the liver and lungs, where it is coughed up and swallowed developing into the adult worm in the intestine. Transmission is aided by poor sanitation or when food crops are manured with human faeces. In warm, moist climates, the eggs can survive for many years in the soil. Hookworm eggs hatch into an infective larva that is able to burrow through intact skin to cause infection.
Gut helminths
These parasites cause disease by competing for nutrients; thus, the severity of symptoms is proportional to the number of worms present (parasite load). Hookworms take blood, leading to irondeficiency anaemia that can be severe. Heavily infected children have poor growth and lowered school performance, which is attributed to micronutrient deficiency, especially with Trichuris infection.
Infection is usually asymptomatic, but heavy Ascaris infection may lead to intestinal obstruction and heavy Trichuris infection to a dysentery-like syndrome.
Diagnosis
The diagnosis is made by examining up to three stool samples for the presence of the characteristic eggs.
Treatment
Intestinal nematodes are treated with albendazole or mebendazole. Improved sanitation is required to control the spread of infection.
Threadworms
Humans are the only host of Enterobius vermicularis. Living in the large intestine, the females migrate to the anus where they lay their eggs on the perianal skin. Symptoms are few; thread-like worms may be found in the faeces or patients may complain of perianal itching, often worse at night. Scratching allows contamination of the fingers with larvae-containing eggs which, when placed in the mouth, initiate a new cycle of infection. Occasionally, Enterobius can be found in the appendix. Diagnosis is made by sending an adhesive-tape swab to the laboratory where D-shaped eggs are seen. Treatment is with mebendazole or piperazine. It is often necessary to treat the whole family, repeating treatment after 2 weeks, and hygiene should also be addressed.
Strongyloides stercoralis larvae are passed in the stools, where they either undergo a free-living cycle in the soil or differentiate into infective larvae that invade another host via intact skin. Inside the human host, they can initiate another development cycle. As a consequence, infection with Strongyloides can be prolonged. Resistance to Strongyloides depends on efficient cell-mediated immunity. Individuals who are infected with human T-cell leukaemia virus 1 (HTLV-1) or are taking steroids are especially susceptible to hyperinfection.
Clinical features
Migrating larvae leave a red, itchy track, which fades after about 48 h. If the patient is given immunosuppressive therapy, uncontrolled multiplication of the Strongyloides may occur, which is characterized by fever, shock and the signs of septicaemia and meningitis.
Diagnosis
Stool culture from multiple specimens may reveal infective larvae. Alternatively, samples of jejunal fluid are examined for the presence of larvae. A sensitive enzyme immunoassay (EIA) technique for serum is available.
Ivermectin is the optimal drug for treatment, with the imidazoles (e.g. albendazole) as alternatives. Relapse occurs in up to 20% of patients. The hyperinfection syndrome is often accompanied by Gram-negative septicaemia, which requires urgent treatment.
Prevention
The risk of infection can be reduced by wearing appropriate footwear to prevent larvae penetrating the skin.
Tapeworms
Taenia spp.
Two Taenia spp. infect humans: the pork worm, T. solium, and the beef worm, T. saginata. Infection is acquired by eating meat from the intermediate hosts that contains the tissue stages of the parasite.
Tapeworms compete for nutrients and infections are usually asymptomatic. Taenia solium can use humans as an intermediate as well as the definitive host. When an individual ingests T. solium eggs, the eggs hatch and disseminate, forming multiple cyst-like lesions in the muscles, skin and brain. These 'measly' lesions, similar in appearance to infected pork meat, are known as cysticercosis. Inflammatory responses to parasitic antigens that leak from cysts in the brain may lead to epileptic seizures.
Diagnosis
This is made by finding characteristic eggs in the patient's stool. Cysticercosis is diagnosed by a specific EIA and confirmed by demonstrating the presence of multiple tissue cysts by X-ray, CT or MRI. br>
Treatment and Prevention
Treatment is with praziquantel. Specialist advice should be sought for the management of Taenia infections in the central nervous system as severe inflammatory reactions can occur.
Humans are the definitive host of this rare tapeworm, acquiring infection from undercooked freshwater fish. The parasite competes for nutrients and causes deficiency of vitamin B12. The Diagnosis is made by detecting the characteristic eggs in faeces and treatment is with praziquantel. Hymenolepis nana Humans are the only host of this small tapeworm. Infection is usually asymptomatic and diagnosis is made by detecting the characteristic eggs in the faeces. Treatment is with praziquantel.
Support our developers




