Herpesviruses I
Herpesviruses I
Herpesviruses I
Classification
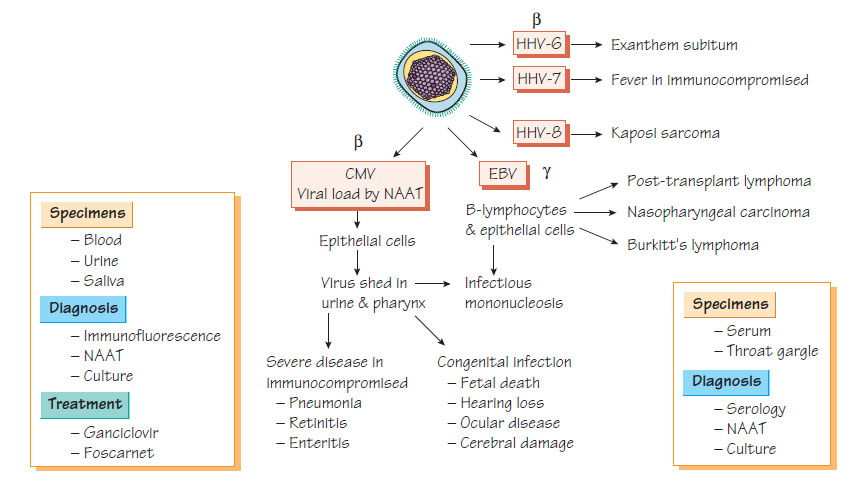
Herpesviruses are divided into three groups:
- α-herpesviruses are fast-growing cytolytic viruses that establish latent infections in neurones (e.g. herpes simplex and varicella zoster);
- β-herpesviruses are slow-growing viruses that become latent in secretory glands and kidneys (e.g. cytomegalovirus [CMV], HHV6 and 7);
- λ-herpesviruses are latent in lymphoid tissues (e.g. Epstein-Barr virus [EBV], HHV-8).
Epidemiology and Pathogenesis
- Transmitted vertically or by close contact.
- Infection occurs later in life with increasing wealth.
- Approximately 50% of adults in the UK have been infected.
- Infection may be transmitted to the fetus before or after birth.
- Infection may also be acquired from blood transfusion or organ transplantation.
Clinical features
- Neonatal infection can be severe (see Congenital and perinatal infections), or may be initially be asymptomatic, later leading to the development of deafness and/or to developmental milestone delay.
- Postnatal infection is usually mild.
- Immunocompromised patients, especially those with HIV infection or who have undergone organ transplantation, may develop severe pneumonitis, retinitis or gut infection through reactivation of latent infection or infection from the donor organ.
- Diagnosis is usually by nucleic acid amplification test (NAAT) on blood, urine or respiratory samples.
- Monitoring of viral load is important to identify patients with severe disease who require treatment.
- The virus is readily cultured.
Treatment and Prevention
- Severe infections that threaten life or sight should be treated with ganciclovir, together with immunoglobulin in the case of pneumonitis.
- Valganciclovir, the ester of ganciclovir, is an oral preparation used for initial treatment and maintenance.
- Alternatives, all of which are more toxic, include foscarnet and cidofovir, a DNA polymerase chain inhibitor.
- Appropriate screening of donor organs and blood products can reduce the risk of transmission.
Epstein-Barr virus
Epidemiology and Pathogenesis
As with CMV, infection is generally found in the very young in developing countries and in adults in industrialized countries. Gaining entry via the pharynx, the virus infects B cells and disseminates widely. EBV is capable of immortalization of B cells causing neoplasia: Burkitt's lymphoma (found in sub-Saharan Africa in association with malaria); nasopharyngeal carcinoma (in China); and lymphoma (in immunocompromised patients including transplant recipients).
- Infection is characterized by fever, malaise, fatigue, sore throat, lymphadenopathy and, occasionally, by hepatitis.
- Symptoms usually last about 2 weeks.
- Persistent symptoms may develop in a few patients.
- EBV infection is associated with tumours (see above).
Diagnosis
- Rapid slide agglutination technique.
- Definitive diagnosis is by detection of specific IgM to EBV viral capsid antigen.
- NAAT-based diagnosis can now also be used.
- The pattern of immune response to Epstein-Barr nuclear antigen complex (EBNA), latent membrane protein, terminal protein, the membrane antigen complex and the early antigen (EA) complex allow the stage of infection to be determined.
- The sole member of the Roseolovirus genus, herpesvirus 6 (HHV-6) has two subtypes, A and B, which infect human T cells.
- Transmission is probably through infected saliva; almost all individuals are infected by the end of their second year.
- The infection, known as 'exanthem subitum', is characterized by a 3 to 5-day febrile illness that settles as the rash appears.
- Asymptomatic infection is common.
- It may be associated with febrile convulsions and encephalitis, although the latter is rare.
- Hepatitis is another rare complication.
- An IgG enzyme immunoassay (EIA) is available and a quantitative NAAT may be helpful in the diagnosis.
- Infection with HHV-7 is almost universal by the age of 5, but there is no clear association with disease.
- Diagnosis is with paired sera to detect antibody levels.
The human Kaposi sarcomavirus (HHV-8) is a λ-herpesvirus. Transmission can be vertical from mother to child, and in the young is by mucosal (non-sexual) contact. Initial infection is characterized by infectious mononucleosis-like syndrome. Later, immunocompromised patients, especially those with AIDS, may develop Kaposi sarcoma. Diagnosis is principally by NAAT in suspect tissues. Serological tests using EIA and indirect fluorescence are available.
Support our developers




