Parainfluenza and other respiratory viruses
Parainfluenza and other respiratory viruses
This is a fragile, enveloped paramyxovirus (150-300 nm) containing a single strand of negative-sense RNA (15 kb). It has four types that share antigenic determinants.
Pathogenesis and Epidemiology
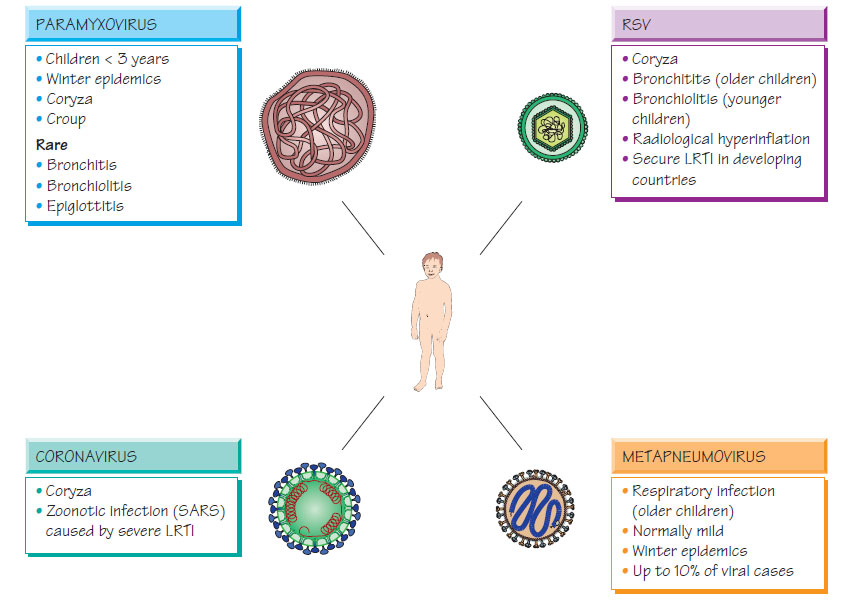
The virus attaches to host cells, where the envelope fuses with the host cell membrane. The virus multiplies throughout the tracheobronchial tree. Infection, which is transmitted by the respiratory route, peaks in the winter, with the highest attack rates occurring in children under 3 years old.
Parainfluenza and other respiratory viruses
In this common, self-limiting condition, which usually lasts 4-5 days, children are distressed, coryzal and febrile. In young children, hoarse coughing often alternates with hoarse crying and is associated with inspiratory stridor secondary to laryngeal obstruction (croup). Rarely, bronchiolitis, bronchopneumonia or acute epiglottitis may develop, signalled by reduced air entry and cyanosis.
Diagnosis and Treatment
Diagnosis is clinical. Direct immunofluorescence gives rapid results; viral isolation and reverse transcriptase nucleic acid amplification tests (NAATs) are available as part of a respiratory virus screen. Treatment is symptomatic (e.g. paracetamol and humidification). Severe infection can be treated with ribavirin and humidified oxygen.
This enveloped paramyxovirus (120-300 nm) containing a single strand of negative-sense RNA attaches to host cells by 12-nm glycoprotein spikes. There is antigenic variation within the two types, designated A and B.
Epidemiology
Respiratory syncytial virus (RSV) is found worldwide, infecting children during the first 3 years of life. There are yearly epidemics in the winter months in temperate countries and in the rainy season in tropical countries. RSV spreads readily in the hospital environment. Patients who are elderly and frail, and those with a compromised respiratory tract can develop serious infection.
Coryza develops after a 4 to 5-day incubation period. In 40% of cases bronchitis develops in older children and bronchiolitis in the very young. Severe disease can develop quickly but, with intensive care, mortality is very low. Children with bronchiolitis are febrile and tachypnoeic, with chest hyperinflation, wheezing and crepitations. Cyanosis is rare. The radiological appearances are variable and include hyperinflation and increased peribronchial markings.
Diagnosis and Treatment
Direct immunofluorescence or enzyme immunoassay (EIA) of nasopharyngeal secretions is rapid. Many laboratories use reverse transcriptase NAAT for diagnosis. The virus can be cultivated. Treatment for RSV infection is based on symptomatic relief and humidification. Severe cases may require hospitalization and humidified oxygen. Severely ill, immunocompromised patients may benefit from aerosolized ribavirin.
Prevention
There is no currently available vaccine.
This is a spherical enveloped virus (80-160 nm) with positive-sense linear single-stranded RNA (27 kb); the envelope contains widely spaced club-shaped spikes. Coronaviruses cause a coryza-like illness similar to that of rhinovirus. The virus has been observed in the faeces of patients with diarrhoeal disease and asymptomatic subjects. Diagnosis is by serology using a complement fixation test (CFT) or EIA, by detection of coronavirus-specific antigens or by electron microscopy. A coronavirus that emerged in China was associated with severe pneumonia (SARS). It was transmitted by the respiratory and oral route; mortality was approximately 10%, but higher in elderly people and patients who were immunocompromised. Healthcare workers were vulnerable to infection, so stringent precautions were required to prevent hospital transmission. Coordinated infection control has permitted eradication of the virus.
Human metapneumovirus, a paramyxovirus, has recently been identified from children with acute respiratory tract infections. It accounts for just under 10% of cases that occur in the winter months, causing a clinical syndrome that is similar to RSV infection. Dual infection with RSV is associated with severe disease. Diagnosis is by reverse transcriptase NAAT.
Support our developers




