Measles, mumps and rubella
Measles, mumps and rubella
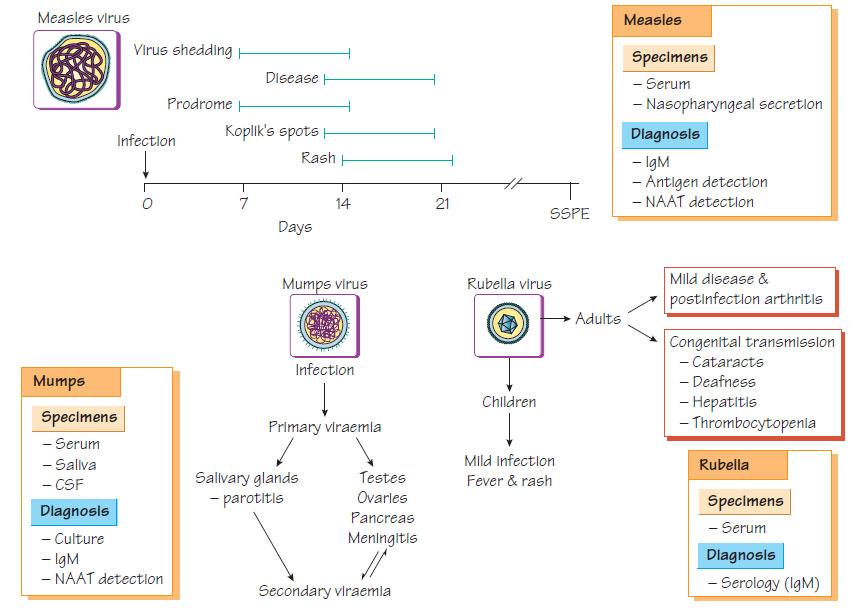
Measles is due to an enveloped RNA virus, known as a Morbillivirus, with a single serotype. The virus encodes six structural proteins that facilitate attachment to the host cell and viral entry, which includes two transmembrane glycoproteins: fusion (F) and haemagglutinin (H). Antibodies to F and H are protective.
Measles, mumps and rubella
- Initially the virus infects epithelial cells of the upper respiratory tract.
- It then invades neighbouring lymphoid tissue, which results in primary viraemia and involvement of the reticuloendothelial system.
- This is followed by a secondary viraemia and dissemination throughout the body, which coincides with the onset of clinical symptoms.
- It is transmitted by the airborne route, with a high attack rate.
- The incubation period is 9-12 days - individuals are infectious for 3 days before the rash emerges.
- Natural infection is followed by lifelong immunity.
- Mortality is rare except in patients who have HIV infection, are immunocompromised or malnourished (especially those with vitamin A deficiency); mortality rates are highest in children under 2 years of age.
- Measles is rare in countries with a vaccination programme but 90% coverage is required to ensure the disease does not re-emerge.
- A prodromal 2 to 4-day coryzal illness occurs, during which small white papules (Koplik's spots) are found on the buccal mucosa near the first premolars.
- A morbilliform rash appears, first behind the ears, then spreading centrifugally and becoming brownish.
- Secondary pneumonia, otitis media and croup are common complications.
- Acute postinfectious encephalitis is a rare and serious complication.
- Subacute encephalitis, a chronic progressive disease, occurs mainly in children with leukaemia.
- Subacute sclerosing panencephalitis (SSPE) is a rare, progressive, fatal encephalitis that develops more than 6 years after infection.
- Diagnosis is usually clinical, but may be confirmed by salivary IgM-specific enzyme immunoassay (EIA).
- SSPE is diagnosed by detection of virus-specific antibody that is being synthesized in the CSF (e.g. specific IgM).
- A nucleic acid amplification test (NAAT) and molecular characterization of the virus by sequencing are also available.
Mumps
A member of the Paramyxovirus genus, the mumps virus is a pleomorphic, enveloped, antisense RNA virus with one serotype.
- Mumps usually occurs in childhood but many adults are susceptible as it has a relatively low attack rate.
- The incubation period is 14-24 days.
- Subclinical infection is common, especially in children.
- It is transmitted readily by the aerial route.
- Infection creates lifelong immunity.
- Epidemics can re-emerge if vaccination coverage falls.
Clinical features
- Common features include fever, malaise, myalgia and parotid gland inflammation.
- Meningitis occurs in up to 15% of patients with parotitis.
- Complete recovery is almost invariable, although rare fatal forms and postmeningitis deafness may occur.
- Complications include orchitis (20%), oophoritis (5%) or pancreatitis (5%) usually in older individuals.
- Diagnosis is usually clinical, but may be confirmed by specific salivary or serum IgM.
- NAAT for diagnosis is also available.
Rubella
Rubella (rubivirus), which is a member of the Togaviridae family, is an icosahedral, pleomorphic, enveloped, positive-strand RNA virus with a single serotype.
Epidemiology
- Rubella is rare in countries with a vaccination programme.
- Transmission is by aerial droplets.
- Patients are infectious from 7 days before the rash appears until 14 days after the rash.
- Natural infection is followed by solid immunity.
Rubella is associated with fever, a fine, red, maculopapular rash and lymphadenopathy. During the prodrome red pinpoint lesions occur on the soft palate. Arthritis (more common in females) and self-limiting encephalitis are complications. Maternal infection may cause fetal death or severe abnormalities, such as deafness, central nervous system deficit, cataract, neonatal purpura and cardiac defects, in up to 60% of cases; the risk being highest during the first trimester.
Diagnosis
- Diagnosis is by detection of IgM and IgG antibodies in serum or saliva.
- Congenital disease is diagnosed by finding specific IgM persistent antibodies (>6 months) in an infant, or viral detection by culture or NAAT.
- A live attenuated combined vaccine (the MMR) is given between 13 and 15 months, with a booster dose given at school entry.
- Further booster doses of measles vaccine may be required.
- The rapid antibody response to measles vaccine can be used to protect susceptible individuals exposed to measles.
- Women attending for contraceptive advice should be screened for rubella antibodies and vaccinated if not pregnant.
- MMR should not be given to immunocompromised individuals.
Support our developers




