Urinary and genital infections
Urinary and genital infections
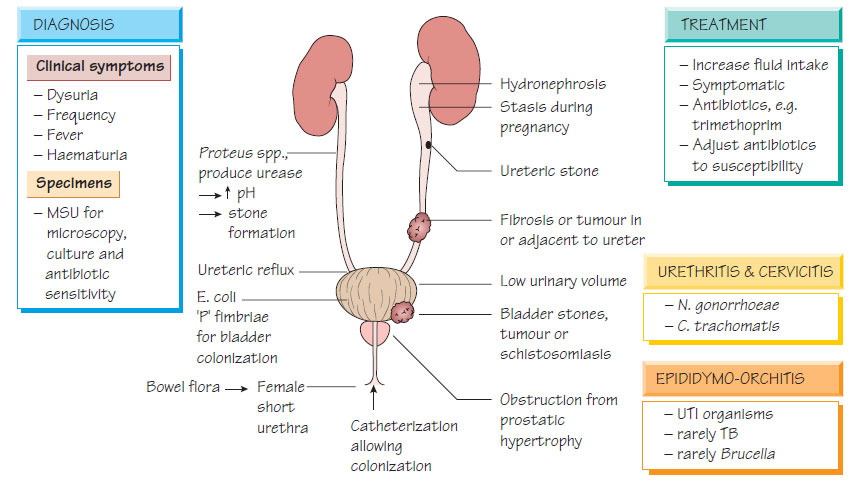
Anatomical considerations
Only the lower part of the urethra is usually colonized by bacteria; the flushing action of urinary flow prevents ascending infection. The shorter female urethra makes urinary infection more common.
Epidemiology and Pathogenesis
Dehydration, obstruction, the disturbance of smooth urinary flow or the presence of a foreign body such as a stone or urinary catheter predisposes to urinary infection. Trauma during sexual intercourse may precipitate infection in women. Infection in children, especially in boys, is often associated with congenital abnormalities, such as ureteric reflux or urethral valves.
Urinary and genital infections
- Lower urinary tract infections: urinary frequency, dysuria and suprapubic discomfort; fever may be absent.
- Pyelonephritis: fever, loin pain, renal angle tenderness and signs of septicaemia.
- Infection in children, elderly people and antenatal patients: may be clinically silent.
- Recurrent infections can result in scarring and renal failure.
Laboratory diagnosis
- 'Dip-stick' test for leukocyte esterase and nitrite can identify patients with infection and the need for treatment without culture.
- Culture using a midstream urine (MSU) specimen to reduce the risk of contamination.
- >105 colony-forming units/mL of a single organism indicate infection, whereas <105 organisms/mL or a mixed growth suggests contamination.
- Chronically catheterized patients usually have 'significant' numbers of organisms and multiple pathogens and may not have active infection.
- All isolates are potentially significant from a suprapubic aspirate from an infant with suspected infection.
- Susceptibility tests should be performed on all significant isolates.
- Empirical therapy is based on the known susceptibilities of urinary pathogens.
- Most community-acquired infections respond to oral antibiotics (e.g. cefalexin, amoxicillin, trimethoprim or nitrofurantoin).
- If septicaemia is present, ciprofloxacin or cefotaxime should be used.
- Recurrent urinary infection may require nocturnal prophylaxis (e.g. low-dose trimethoprim, nitrofurantoin or naladixic acid), together with advice on ensuring an adequate urine flow is achieved.
- Children with recurrent infection should be investigated for anatomical abnormalities.
- Significant bacteriuria in pregnant women should be treated, even if asymptomatic.
- Anatomical obstructions to urine flow should be removed if possible.
Genital infection
Genital infection presents in many ways (see Table). It may be followed by pelvic inflammatory disease, infertility, prostatitis, arthritis or bacteraemia. Other sites may be involved, for example the throat and rectum in gonococcal infection.
| Genitourinary infection syndromes and causative organisms. | |
| Syndrome | Organisms |
| Genital ulcers | Herpes simplex Chlamydia trachomatis types L1–4 Haemophilus ducreyi (see Small Gram-negative coccobacilli: Haemophilus, Brucella, Francisella, Yersinia and Bartonella) Treponema pallidum (see Spiral bacteria) Calymmatobacterium donovani |
| Urethral discharge | Neisseria gonorrhoeae C. trachomatis |
| Pelvic inflammatory disease | N. gonorrhoeae C. trachomatis Mixed anaerobic infection |
| Vaginal discharge | Candida albicans Trichomonas vaginalis Mobiluncus spp. and others in non-specific vaginitis |
Urethral and cervical swabs should be taken for both bacterial and viral diagnosis. N. gonorrhoeae, Chlamydia and herpes simplex are optimally detected by nucleic acid amplification tests (NAATs; see Chlamydia, Mycoplasma and Rickettsia and Herpesviruses II). Samples positive for N. gonorrhoeae can be cultured for susceptibility testing. Syphilis is diagnosed with enzyme immunoassay (EIA) together with traditional treponemal tests (see Spiral bacteria). Direct microscopy may show evidence of Candida or Trichomonas.
Treatment
Patients must be treated before a laboratory diagnosis, so Treatment is guided by a 'syndromic approach' where therapy is based on the agents that are likely to treat at least 95% of organisms in a community. For example, patients with uncomplicated urethritis can be treated with a single dose of a suitable cephalosporin or fluoroquinolone followed by a 1-week course of either doxycycline or single-dose azithromycin. Syphilis is treated with penicillin (see Spiral bacteria).
- Risk avoidance (e.g. monogamous relationships).
- Risk reduction (e.g. barrier contraceptive methods).
- Tracing of sexual contacts to treat asymptomatic disease.
- Antigen variability in N. gonorrhoeae means that there is no effective vaccine for gonorrhoea.
Trichomonas vaginalis
- Causes an itchy vaginal infection with an offensive discharge.
- Treatment of sexual contacts may be necessary to prevent recurrent infection.
Non-specific vaginosis
- Caused by disruption to the normal vaginal flora.
- Results in an offensive discharge with a characteristic fishy smell when alkalinized.
- Diagnosis is based on clinical findings and near-patient tests (e.g. 'clue cells', which are epithelial cells heavily coated with bacteria, and a positive amine test) and defined syndrome scoring schemes.
- Clindamycin preparations, oral metronidazole, and oral and intravaginal tablets of lactobacillus are effective treatments.
Infection of the epididymis may arise (i) from a urinary tract infection, (ii) as part of a genital infection or (iii) as a primary systemic infection, such as brucellosis or tuberculosis. Patients present with a painful, acutely inflamed epididymis and testis, which must be differentiated from testicular torsion. Diagnosis is made clinically and confirmed by the result of urinary or blood cultures and tests for sexually transmitted infections.
Support our developers




